 |
Prescribing Information as of February 1999
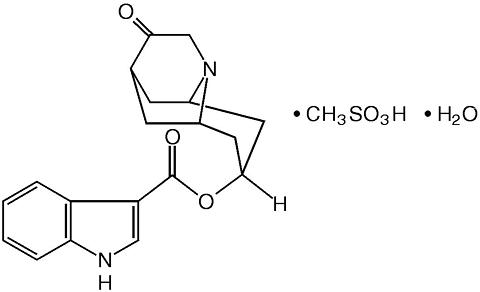
ANZEMET (dolasetron mesylate) is an antinauseant and antiemetic agent. Chemically, dolasetron mesylate is (2(alpha),6(alpha),8(alpha),9a(beta))-octahydro-3-oxo-2,6-methano-2 H -quinolizin-8-yl-l H -indole-3-carboxylate monomethanesulfonate, monohydrate. It is a highly specific and selective serotonin subtype 3 (5-HT 3 ) receptor antagonist both in vitro and in vivo. Dolasetron mesylate has the following structural formula:
|
|
The empirical formula is C 19 H 20 N 2 O 3 · CH 3 SO 3 H · H 2 O, with a molecular weight of 438.50. Approximately 74% of dolasetron mesylate monohydrate is dolasetron base.
Dolasetron mesylate monohydrate is a white to off-white powder that is freely soluble in water and propylene glycol, slightly soluble in ethanol, and slightly soluble in normal saline.
ANZEMET Injection is a clear, colorless, nonpyrogenic, sterile solution for intravenous administration. Each milliliter of ANZEMET Injection contains 20 mg of dolasetron mesylate and 38.2 mg mannitol with an acetate buffer in water for injection. The pH of the resulting solution is 3.2 to 3.8.
Dolasetron mesylate and its active metabolite, hydrodolasetron (MDL 74,156), are selective serotonin 5-HT 3 receptor antagonists not shown to have activity at other known serotonin receptors and with low affinity for dopamine receptors. The serotonin 5-HT 3 receptors are located on the nerve terminals of the vagus in the periphery and centrally in the chemoreceptor trigger zone of the area postrema. It is thought that chemotherapeutic agents produce nausea and vomiting by releasing serotonin from the enterochromaffin cells of the small intestine, and that the released serotonin then activates 5-HT 3 receptors located on vagal efferents to initiate the vomiting reflex.
Acute, usually reversible, ECG changes (PR and QT c prolongation; QRS widening), caused by dolasetron mesylate, have been observed in healthy volunteers and in controlled clinical trials. The active metabolites of dolasetron may block sodium channels, a property unrelated to its ability to block 5-HT 3 receptors. QT c prolongation is primarily due to QRS widening. Dolasetron appears to prolong both depolarization and, to a lesser extent, repolarization time. The magnitude and frequency of the ECG changes increased with dose (related to peak plasma concentrations of hydrodolasetron but not the parent compound). These ECG interval prolongations usually returned to baseline within 6 to 8 hours, but in some patients were present at 24 hour follow up. Dolasetron mesylate administration has little or no effect on blood pressure.
In healthy volunteers (N=64), dolasetron mesylate in single intravenous doses up to 5 mg/kg produced no effect on pupil size or meaningful changes in EEG tracings. Results from neuropsychiatric tests revealed that dolasetron mesylate did not alter mood or concentration. Multiple daily doses of dolasetron have had no effect on colonic transit in humans. Dolasetron mesylate has no effect on plasma prolactin concentrations.
Intravenous dolasetron mesylate is rapidly eliminated (t ½ <10 min) and completely metabolized to the most clinically relevant species, hydrodolasetron.
The reduction of dolasetron to hydrodolasetron is mediated by a ubiquitous enzyme, carbonyl reductase. Cytochrome P-450 (CYP)IID6 is primarily responsible for the subsequent hydroxylation of hydrodolasetron and both CYPIIIA and flavin monooxygenase are responsible for the N-oxidation of hydrodolasetron.
Hydrodolasetron is excreted in the urine unchanged (53.0% of administered intravenous dose). Other urinary metabolites include hydroxylated glucuronides and N-oxide.
Hydrodolasetron appeared rapidly in plasma, with a maximum concentration occurring approximately 0.6 hour after the end of intravenous treatment, and was eliminated with a mean half-life of 7.3 hours (%CV=24) and an apparent clearance of 9.4 mL/min/kg (%CV=28) in 24 adults. Hydrodolasetron is eliminated by multiple routes, including renal excretion and, after metabolism, mainly glucuronidation, and hydroxylation. Hydrodolasetron exhibits linear pharmacokinetics over the intravenous dose range of 50 to 200 mg and they are independent of infusion rate. Doses lower than 50 mg have not been studied. Two thirds of the administered dose is recovered in the urine and one third in the feces. Hydrodolasetron is widely distributed in the body with a mean apparent volume of distribution of 5.8 L/kg (%CV=25, N=24) in adults.
Sixty-nine to 77% of hydrodolasetron is bound to plasma protein. In a study with 14 C labeled dolasetron, the distribution of radioactivity to blood cells was not extensive. The binding of hydrodolasetron to (alpha) 1 -acid glycoprotein is approximately 50%. The pharmacokinetics of hydrodolasetron are linear and similar in men and women.
The pharmacokinetics of hydrodolasetron, in special and targeted patient populations following intravenous administration of ANZEMET Injection, are summarized in Table 1. The pharmacokinetics of hydrodolasetron are similar in adult healthy volunteers and in adult cancer patients receiving chemotherapeutic agents. The apparent clearance of hydrodolasetron in pediatric and adolescent patients is 1.4 times to twofold higher than in adults. The apparent clearance of hydrodolasetron is not affected by age in adult cancer patients. Following intravenous administration, the apparent clearance of hydrodolasetron remains unchanged with severe hepatic impairment and decreases 47% with severe renal impairment. No dose adjustment is necessary for elderly patients or for patients with hepatic or renal impairment.
In a pharmacokinetic study in pediatric cancer patients (ages 3 to 11, N=25; ages 12 to 17, N=21) given a single 0.6, 1.2, 1.8, or 2.4 mg/kg dose of ANZEMET Injection intravenously, apparent clearance values were highest and half-lives were lowest in the youngest age group. For the 3 to 11 and the 12 to 17 year age groups, all receiving doses between 0.6 to 2.4 mg/kg, mean apparent clearances are 2 and 1.3 times greater, respectively, than for healthy adults receiving the same range of doses.
Thirty-two pediatric cancer patients ages 3 to 11 years (N=19) and 12 to 17 years (N=13), received 0.6, 1.2, or 1.8 mg ANZEMET Injection diluted with either apple or apple-grape juice and administered orally. In this study, the mean apparent clearances were 3 times greater in the younger pediatric group and 1.8 times greater in the older pediatric group than those observed in healthy adult volunteers. Across this spectrum of pediatric patients, maximum plasma concentrations were 0.6 to 0.7 times those observed in healthy adults receiving similar doses.
In a pharmacokinetic study in 18 pediatric patients (2 to 11 years of age) undergoing surgery with general anesthesia and administered a single 1.2 mg/kg intravenous dose of ANZEMET Injection, mean apparent clearance was greater (40%) and terminal half-life shorter (36%) for hydrodolasetron than in healthy adults receiving the same dose.
For 12 pediatric patients, ages 2 to 12 years receiving 1.2 mg/kg ANZEMET Injection diluted in apple or apple-grape juice and administered orally, the mean apparent clearance was 34% greater and half-life was 21% shorter than in healthy adults receiving the same dose.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
ANZEMET Injection administered intravenously at a dose of 1.8 mg/kg gave similar results in preventing nausea and vomiting as the other selective serotonin 5-HT 3 receptor antagonists studied as active comparators. It was more effective than metoclopramide. Efficacy was based on complete response rates (0 emetic episodes and no rescue medication).
A randomized, double-blind trial compared single intravenous doses of ANZEMET Injection with metoclopramide in 226 (160 men and 66 women) adult cancer patients receiving >/=80 mg/m 2 cisplatin. ANZEMET Injection at a dose of 1.8 mg/kg was significantly more effective than metoclopramide in the prevention of chemotherapy-induced nausea and vomiting in this study (Table 2).
|
||||||||||||||||||||||||||||||||||||||||
A second randomized, double-blind trial compared single intravenous doses of ANZEMET Injection with intravenous ondansetron in 609 (377 men and 232 women) adult cancer patients receiving >/=70 mg/m 2 cisplatin. A single intravenous 1.8 mg/kg dose of ANZEMET Injection was shown to be equivalent to a single intravenous 32 mg dose of ondansetron (Table 3).
|
||||||||||||||||||||||||||||||||||||||||
Another randomized, double-blind trial compared single IV doses of ANZEMET with a single 3-mg IV dose of granisetron in 474 (315 men and 159 women) patients receiving >/=80 mg/m 2 cisplatin chemotherapy. A single intravenous 1.8-mg/kg dose of ANZEMET gave similar results as those from granisetron.
In a study of ANZEMET Injection in 309 patients (96 men and 213 women) receiving moderately emetogenic chemotherapy such as cyclophosphamide based regimens, a single intravenous 1.8 mg/kg dose of ANZEMET Injection was equivalent to metoclopramide administered as a 2 mg/kg intravenous bolus followed by 3 mg/kg intravenously over 8 hours. Complete response rates were 63% and 52%, respectively, p=0.12.
ANZEMET Injection administered intravenously at a dose of 12.5 mg approximately 15 minutes before the cessation of general balanced anesthesia (short-acting barbiturate, nitrous oxide, narcotic and analgesic, and skeletal muscle relaxant) was significantly more effective than placebo in preventing postoperative nausea and vomiting. No increased efficacy was seen with higher doses.
One trial compared single intravenous ANZEMET Injection doses of 12.5, 25, 50, and 100 mg with placebo in 635 women surgical patients undergoing laparoscopic procedures. ANZEMET Injection at a dose of 12.5 mg was statistically superior to placebo for complete response (no vomiting, no rescue medication) (p=.0003). Complete response rates were 50% and 31%, respectively.
Another trial compared single intravenous ANZEMET Injection doses of 12.5, 25, 50, and 100 mg with placebo in 1030 (722 women and 308 men) surgical patients. In women, the 12.5 mg dose was statistically superior to placebo for complete response. The complete response rates were 50% and 40%, respectively. However, in men, there was no statistically significant difference in complete response between any ANZEMET dose and placebo.
Two randomized, double-blinded trials compared single intravenous ANZEMET Injection doses of 12.5, 25, 50, and 100 mg with placebo in 124 male and 833 female patients who had undergone surgery with general balanced anesthesia and presented with early postoperative nausea or vomiting requiring antiemetic treatment.
In both studies, the 12.5 mg intravenous dose of ANZEMET was statistically superior to placebo for complete response (no vomiting, no escape medication). No significant increased efficacy was seen with higher doses.
ANZEMET Injection is indicated for the following:
ANZEMET Injection is contraindicated in patients known to have hypersensitivity to the drug.
ANZEMET can cause ECG interval changes (PR, QT c , JT prolongation and QRS widening). These changes are related in magnitude and frequency to blood levels of the active metabolite. These changes are self-limiting with declining blood levels. Some patients have interval prolongations for 24 hours or longer. Interval prolongation could lead to cardiovascular consequences, including heart block or cardiac arrhythmias. These have rarely been reported.
A cardiac conduction abnormality observed on an intra-operative cardiac rhythm monitor (interpreted as complete heart block) was reported in a 61-year-old woman who received 200 mg ANZEMET for the prevention of postoperative nausea and vomiting. This patient was also taking verapamil. A similar event also interpreted as complete heart block was reported in one patient receiving placebo.
A 66-year-old man with Stage IV non-Hodgkins lymphoma died suddenly 6 hours after receiving 1.8 mg/kg (119 mg) intravenous ANZEMET Injection. This patient had other potential risk factors including substantial exposure to doxorubicin and concomitant cyclophosphamide.
Dolasetron should be administered with caution in patients who have or may develop prolongation of cardiac conduction intervals, particularly QT c . These include patients with hypokalemia or hypomagnesemia, patients taking diuretics with potential for inducing electrolyte abnormalities, patients with congenital QT syndrome, patients taking anti-arrhythmic drugs or other drugs which lead to QT prolongation, and cumulative high dose anthracycline therapy.
Cross hypersensitivity reactions have been reported in patients who received other selective 5-HT 3 receptor antagonists. These reactions have not been seen with dolasetron mesylate.
The potential for clinically significant drug-drug interactions posed by dolasetron and hydrodolasetron appears to be low for drugs commonly used in chemotherapy or surgery, because hydrodolasetron is eliminated by multiple routes. See PRECAUTIONS, General for information about potential interaction with other drugs that prolong the QT c interval. Blood levels of hydrodolasetron increased 24% when dolasetron was coadministered with cimetidine (nonselective inhibitor of cytochrome P-450) for 7 days, and decreased 28% with coadministration of rifampin (potent inducer of cytochrome P-450) for 7 days.
ANZEMET Injection has been safely coadministered with drugs used in chemotherapy and surgery. As with other agents which prolong ECG intervals, caution should be exercised in patients taking drugs which prolong ECG intervals, particularly QT c .
In patients taking furosemide, nifedipine, diltiazem, ACE inhibitors, verapamil, glyburide, propranolol, and various chemotherapy agents, no effect was shown on the clearance of hydrodolasetron. Clearance of hydrodolasetron decreased by about 27% when dolasetron mesylate was administered intravenously concomitantly with atenolol. ANZEMET did not influence anesthesia recovery time in patients. Dolasetron mesylate did not inhibit the antitumor activity of four chemotherapeutic agents (cisplatin, 5-fluorouracil, doxorubicin, cyclophosphamide) in four murine models.
In a 24-month carcinogenicity study, there was a statistically significant (P<0.001) increase in the incidence of combined hepatocellular adenomas and carcinomas in male mice treated with 150 mg/kg/day and above. In this study, mice (CD-1) were treated orally with dolasetron mesylate 75, 150 or 300 mg/kg/day (225, 450 or 900 mg/m 2 /day). For a 50 kg person of average height (1.46 m 2 body surface area), these doses represent 3.4, 6.8 and 13.5 times the recommended clinical dose (66.6 mg/m 2 , intravenous) on a body surface area basis. No increase in liver tumors was observed at a dose of 75 mg/kg/day in male mice and at doses up to 300 mg/kg/day in female mice.
In a 24-month rat (Sprague-Dawley) carcinogenicity study, oral dolasetron mesylate was not tumorigenic at doses up to 150 mg/kg/day (900 mg/m 2 /day, 13.5 times the recommended human dose based on body surface area) in male rats and 300 mg/kg/day (1800 mg/m 2 /day, 27 times the recommended human dose based on body surface area) in female rats.
Dolasetron mesylate was not genotoxic in the Ames test, the rat lymphocyte chromosomal aberration test, the Chinese hamster ovary (CHO) cell (HGPRT) forward mutation test, the rat hepatocyte unscheduled DNA synthesis (UDS) test or the mouse micronucleus test.
Dolasetron mesylate was found to have no effect on fertility and reproductive performance at oral doses up to 100 mg/kg/day (600 mg/m 2 /day, 9 times the recommended human dose based on body surface area) in female rats and up to 400 mg/kg/day (2400 mg/m 2 /day, 36 times the recommended human dose based on body surface area) in male rats.
Teratology studies have not revealed evidence of impaired fertility or harm to the fetus due to dolasetron mesylate. These studies have been performed in pregnant rats at intravenous doses up to 60 mg/kg/day (5.4 times the recommended human dose based on body surface area) and pregnant rabbits at intravenous doses up to 20 mg/kg/day (3.2 times the recommended human dose based on body surface area). There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
It is not known whether dolasetron mesylate is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when ANZEMET Injection is administered to a nursing woman.
Four open-label, noncomparative pharmacokinetic studies have been performed in a total of 108 pediatric patients receiving emetogenic chemotherapy or undergoing surgery with general anesthesia. These patients received ANZEMET Injection either intravenously or orally in juice. Pediatric patients from 2 to 17 years of age participated in these trials, which included intravenous ANZEMET Injection doses of 0.6, 1.2, 1.8, or 2.4 mg/kg, and oral doses of 0.6, 1.2, or 1.8 mg/kg. There is no experience in pediatric patients under 2 years of age. Overall, ANZEMET Injection was well tolerated in these pediatric patients. Efficacy information collected in pediatric patients receiving cancer chemotherapy are consistent with those obtained in adults. No efficacy information was collected in the pediatric postoperative nausea and vomiting studies.
Dosage adjustment is not needed in patients over 65. Effectiveness in prevention of nausea and vomiting in elderly patients was no different than in younger age groups.
In controlled clinical trials, 2265 adult patients received ANZEMET Injection. The overall adverse event rates were similar with 1.8 mg/kg ANZEMET Injection and ondansetron or granisetron. Patients were receiving concurrent chemotherapy, predominantly high-dose (>/=50 mg/m 2 ) cisplatin. Following is a combined listing of all adverse events reported in >/=2% of patients in these controlled trials (Table 4).
|
|||||||||||||||||||||||||||||||||||||||
In controlled clinical trials with 2550 adult patients, headache and dizziness were reported more frequently with 12.5 mg ANZEMET Injection than with placebo. Rates of other adverse events were similar. Following is a listing of all adverse events reported in >/=2% of patients receiving either placebo or 12.5 mg ANZEMET Injection for the prevention or treatment of postoperative nausea and vomiting in controlled clinical trials (Table 5).
|
In clinical trials, the following infrequently reported adverse events, assessed by investigators as treatment-related or causality unknown, occurred following oral or intravenous administration of ANZEMET to adult patients receiving concomitant cancer chemotherapy or surgery:
Cardiovascular: Hypotension; rarely-edema, peripheral edema. The following events also occurred rarely and with a similar frequency as placebo and/or active comparator: Mobitz I AV block, chest pain, orthostatic hypotension, myocardial ischemia, syncope, severe bradycardia, and palpitations. See PRECAUTIONS section for information on potential effects on ECG.
In addition, the following asymptomatic treatment-emergent ECG changes were seen at rates less than or equal to those for active or placebo controls: bradycardia, tachycardia, T wave change, ST-T wave change, sinus arrhythmia, extrasystole (APCs or VPCs), poor R-wave progression, bundle branch block (left and right), nodal arrhythmia, U wave change, atrial flutter/fibrillation.
Furthermore, severe hypotension, bradycardia and syncope have been reported immediately or closely following IV administration.
Dermatologic: Rash, increased sweating.
Gastrointestinal System: Constipation, dyspepsia, abdominal pain, anorexia; rarely-pancreatitis.
Hearing, Taste and Vision: Taste perversion, abnormal vision; rarely-tinnitus, photophobia.
Hematologic: Rarely-hematuria, epistaxis, prothrombin time prolonged, PTT increased, anemia, purpura/hematoma, thrombocytopenia.
Hypersensitivity: Rarely-anaphylactic reaction, facial edema, urticaria.
Liver and Biliary System: Transient increases in AST (SGOT) and/or ALT (SGPT) values have been reported as adverse events in less than 1% of adult patients receiving ANZEMET in clinical trials. The increases did not appear to be related to dose or duration of therapy and were not associated with symptomatic hepatic disease. Similar increases were seen with patients receiving active comparator. Rarely-hyperbilirubinemia, increased GGT.
Metabolic and Nutritional: Rarely-alkaline phosphatase increased.
Musculoskeletal Rarely-myalgia, arthralgia.
Nervous System: Flushing, vertigo, paraesthesia, tremor; rarely-ataxia, twitching.
Psychiatric Agitation, sleep disorder, depersonalization; rarely-confusion, anxiety, abnormal dreaming.
Respiratory System: Rarely-dyspnea, bronchospasm.
Urinary System: Rarely-dysuria, polyuria, acute renal failure.
Vascular (Extracardiac): Local pain or burning on IV administration; rarely-peripheral ischemia, thrombophlebitis/phlebitis.
A 59-year-old man with metastatic melanoma and no known pre-existing cardiac conditions developed severe hypotension and dizziness 40 minutes after receiving a 15 minute intravenous infusion of 1000 mg (13 mg/kg) of dolasetron mesylate. Treatment for the overdose consisted of infusion of 500 mL of a plasma expander, dopamine, and atropine. The patient had normal sinus rhythm and prolongation of PR, QRS and QT c intervals on an ECG recorded 2 hours after the infusion. The patient' blood pressure was normal 3 hours after the event and the ECG intervals returned to baseline on follow-up. The patient was released from the hospital 6 hours after the event.
Following a suspected overdose of ANZEMET Injection, a patient found to have second-degree or higher AV conduction block with ECG should undergo cardiac telemetry monitoring.
There is no known specific antidote for dolasetron mesylate, and patients with suspected overdose should be managed with supportive therapy. Individual doses as large as 5 mg/kg intravenously or 400 mg orally have been safely given to healthy volunteers or cancer patients.
It is not known if dolasetron mesylate is removed by hemodialysis or peritoneal dialysis.
A 7-year-old boy received 6 mg/kg dolasetron mesylate orally before surgery. No symptoms occurred and no treatment was required.
Single intravenous doses of dolasetron mesylate at 160 mg/kg in male mice and 140 mg/kg in female mice and rats of both sexes (6.3 to 12.6 times the recommended human dose based on body surface area) were lethal. Symptoms of acute toxicity were tremors, depression and convulsions.
The recommended dose of ANZEMET Injection should not be exceeded.
Adults: The recommended intravenous dosage of ANZEMET Injection from clinical trial results is 1.8 mg/kg given as a single dose approximately 30 minutes before chemotherapy (see Administration ). Alternatively, for most patients, a fixed dose of 100 mg can be administered over 30 seconds.
Pediatric Patients: The recommended intravenous dosage in pediatric patients 2 to 16 years of age is 1.8 mg/kg given as a single dose approximately 30 minutes before chemotherapy, up to a maximum of 100 mg (see Administration ). Safety and effectiveness in pediatric patients under 2 years of age have not been established.
ANZEMET Injection mixed in apple or apple-grape juice may be used for oral dosing of pediatric patients. When ANZEMET Injection is administered orally, the recommended dosage in pediatric patients 2 to 16 years of age is 1.8 mg/kg up to a maximum 100 mg dose given within 1 hour before chemotherapy.
The diluted product may be kept up to 2 hours at room temperature before use.
Use in the Elderly, in Renal Failure Patients, or in Hepatically Impaired Patients: No dosage adjustment is recommended.
Adults: The recommended intravenous dosage of ANZEMET Injection is 12.5 mg given as a single dose approximately 15 minutes before the cessation of anesthesia (prevention) or as soon as nausea or vomiting presents (treatment).
Pediatric Patients: The recommended intravenous dosage in pediatric patients 2 to 16 years of age is 0.35 mg/kg, with a maximum dose of 12.5 mg, given as a single dose approximately 15 minutes before the cessation of anesthesia or as soon as nausea or vomiting presents. Safety and effectiveness in pediatric patients under 2 years of age have not been established.
ANZEMET Injection mixed in apple or apple-grape juice may be used for oral dosing of pediatric patients. When ANZEMET Injection is administered orally, the recommended oral dosage in pediatric patients 2 to 16 years of age is 1.2 mg/kg up to a maximum 100-mg dose given within 2 hours before surgery. The diluted product may be kept up to 2 hours at room temperature before use.
Use in the Elderly, in Renal Failure Patients, or in Hepatically Impaired Patients: No dosage adjustment is recommended.
ANZEMET Injection can be safely infused intravenously as rapidly as 100 mg/30 seconds or diluted in a compatible intravenous solution (see below) to 50 mL and infused over a period of up to 15 minutes. ANZEMET Injection should not be mixed with other drugs. Flush the infusion line before and after administration of ANZEMET Injection.
After dilution, ANZEMET Injection is stable under normal lighting conditions at room temperature for 24 hours or under refrigeration for 48 hours with the following compatible intravenous fluids: 0.9% sodium chloride injection, 5% dextrose injection, 5% dextrose and 0.45% sodium chloride injection, 5% dextrose and Lactated Ringer' injection, Lactated Ringer' injection, and 10% mannitol injection. Although ANZEMET Injection is chemically and physically stable when diluted as recommended, sterile precautions should be observed because diluents generally do not contain preservative. After dilution, do not use beyond 24 hours, or 48 hours if refrigerated.
Parenteral drug products should be inspected visually for particulate matter and discoloration before administration whenever solution and container permit.
ANZEMET Injection (dolasetron mesylate injection) is supplied in single-use ampuls and vials as a clear, colorless solution.
|
||||||||||||
Store at controlled room temperature 20-25°C (68-77°F). Protect from light.
Prescribing information as of February 1999
Manufactured for Hoechst Marion Roussel, Inc.
Kansas City, MO 64137 USA
Manufactured by Ben Venue Laboratories, Inc.
Bedford, OH 44146 USA
 |