 |
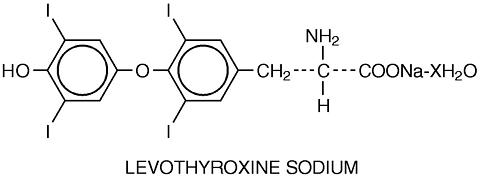
SYNTHROID (levothyroxine sodium, USP) Tablets and Injection contain synthetic crystalline L-3,3',5,5',-tetraiodothyronine sodium salt [levothyroxine (T 4 ) sodium]. Synthetic T 4 is identical to that produced in the human thyroid gland.
Levothyroxine (T 4 ) Sodium has an empirical formula of C 15 H 10 L 4 NNaO 4 xH 2 O, molecular weight of 798.86 (anhydrous), and structural formula as shown:
|
|
Inactive Ingredients (SYNTHROID Tablets): acacia, confectioner's sugar (contains corn starch), lactose, magnesium stearate, providone, talc. The following are the color additives by tablet strength:
|
Inactive Ingredients (SYNTHROID Injection): 10 mg mannitol USP, 0.7 mg tribasic sodium phosphate, anhydrous (200 mcg/vial), 1.75 mg tribasic sodium phosphate, anhydrous (500 mcg/vial), sodium hydroxide, Q.S. for pH adjustment.
Levothyroxine sodium powder for reconstitution for injection is a sterile preparation.
The synthesis and secretion of the major thyroid hormones, L-thyroxine (T 4 ) and L-triiodothyronine (T 3 ), from the normally functioning thyroid gland are regulated by complex feedback mechanisms of the hypothalamic-pituitary-thyroid axis. The thyroid gland is stimulated to secrete thyroid hormones by the action of thyrotropin (thyroid stimulating hormone, TSH), which is produced in the anterior pituitary gland. TSH secretion is in turn controlled by thyrotropin-releasing hormone (TRH) produced in the hypothalamus, circulating thyroid hormones, and possibly other mechanisms. Thyroid hormones circulating in the blood act as feedback inhibitors of both TSH and TRH secretion. Thus, when serum concentrations of T 3 and T 4 are increased, secretion of TSH and TRH decreases. Conversely, when serum thyroid hormone concentrations are decreased, secretion of TSH and TRH is increased. Administration of exogenous thyroid hormones to euthyroid individuals results in suppression of endogenous thyroid hormone secretion.
The mechanisms by which thyroid hormones exert their physiologic actions have not been completely elucidated. T 4 and T 3 are transported into cells by passive and active mechanisms. T 3 in cell cytoplasm and T 3 generated from T 4 within the cell diffuse into the nucleus and bind to thyroid receptor proteins, which appear to be primarily attached to DNA. Receptor binding leads to activation or repression of DNA transcription, thereby altering the amounts of mRNA and resultant proteins. Changes in protein concentrations are responsible for the metabolic changes observed in organs and tissues.
Thyroid hormones enhance oxygen consumption of most body tissues and increase the basal metabolic rate and metabolism of carbohydrates, lipids, and proteins. Thus, they exert a profound influence on every organ system and are of particular importance in the development of the central nervous system. Thyroid hormones also appear to have direct effects on tissues, such as increased myocardial contractility and decreased systemic resistance.
The physiologic effects of thyroid hormones are produced primarily by T 3 , a large portion of which is derived from the deiodination of T 4 in peripheral tissues. About 70 to 90 percent of peripheral T 3 is produced by monodeiodination of T 4 at the 5 position (inner ring) results in the formation of reverse triiodothyronine (rT 3 ), which is calorigenically inactive.
PHARMACOKINETICS Few clinical studies have evaluated the kinetics of orally administered thyroid hormone. In animals, the most active sites of absorption appear to be the proximal and mid-jejunum. T 4 is not absorbed from the stomach and little, if any, drug is absorbed from the duodenum. There seems to be no absorption of T 4 from the distal colon in animals. A number of human studies have confirmed the importance of an intact jejunum and ileum for T 4 absorption and have shown some absorption from the duodenum. Studies involving radioiodinated T 4 fecal excretion methods, equilibration, and AUC methods have shown that absorption varies from 48 to 80 percent of the administered dose. The extent of absorption is increased in the fasting state and decreased in malabsorption syndromes, such as sprue. Absorption may also decrease with age. The degree of T 4 absorption is dependent on the product formulation as well as on the character of the intestinal contents, including plasma protein and soluble dietary factors, which bind thyroid hormone making if unavailable for diffusion. Decreased absorption may result from administration of infant soybean formula, ferrous sulfate, sodium polystyrene sulfonate, aluminum hydroxide, sucralfate or bile acid sequestrants. T 4 absorption following intramuscular administration is variable.
Distribution of thyroid hormones in human body tissues and fluids has not been fully elucidated. More than 99 percent of circulating hormones is bound to serum proteins, including thyroxine-binding globulin (TBG), thyroxine-binding prealbumin (TBPA), and albumin (TBA). T 4 is more extensively and firmly bound to serum proteins than is T 3 . Only unbound thyroid hormone is metabolically active. The higher affinity of TBG and TBPA for T 4 partly explains the higher serum levels, slower metabolic clearance, and longer serum elimination half-life of this hormone.
Certain drugs and physiologic conditions can alter the binding of thyroid hormones to serum proteins and/or the concentrations of the serum proteins available for thyroid hormone binding. These effects must be considered when interpreting the results of thyroid function tests. (See Drug Interactions and Laboratory Test Interactions.)
T 4 is eliminated slowly from the body, with a half-life of 6 to 7 day. T 3 has a half-life of 1 to 2 days. The liver is the major site of degradation for both hormones. T 4 and T 3 are conjugated with glucuronic and sulfuric acids and excreted in the bile. There is an enterohepatic circulation of thyroid hormones, as they are liberated by hydrolysis in the intestine and reabsorbed. A portion of the conjugated material reaches the colon unchanged, is hydrolyzed there, and is eliminated as free compounds in the feces. In man, approximately 20 to 40 percent of T 4 is eliminated in the stool. About 70 percent of the T 4 secreted daily is deiodinated to yield equal amounts of T 3 and rT 3 . Subsequent deiodination of T 3 and rT 4 yields multiple forms of diiodothyronine. A number of the minor T 4 metabolites have also been identified. Although some of these metabolites have biologic activity, their overall contribution to the therapeutic effect of T 4 is minimal.
SYNTHROID is indicated:
SYNTHROID is contraindicated in patients with untreated thyrotoxicosis of any etiology or an apparent hypersensitivity to thyroid hormones or any of the inactive product constituents. (The 50 mcg tablet is formulated without color additives for patients who are sensitive to dyes.) There is no well-documented evidence of true allergic or idiosyncratic reactions to thyroid hormone. SYNTHROID is also contraindicated in the patients with uncorrected adrenal insufficiency, as thyroid hormones increase tissue demands for adrenocortical hormones and may thereby precipitate acute adrenal crisis ( see PRECAUTIONS ).
| : Thyroid hormones, either alone or together with other therapeutic agents, should not be used for the treatment of obesity. In euthyroid patients, doses within the range of daily hormonal requirements are ineffective for weight reduction. Larger doses may produce serious or even life threatening manifestations of toxicity, particularly when given in association with sympathomimetic amines such as those used for their anorectic effects. |
The use of SYNTHROID in the treatment of obesity, either alone or in combination with other drugs, is unjustified. The use of SYNTHROID is also unjustified in the treatment of male or female infertility unless this condition is associated with hypothyroidism.
General: SYNTHROID should be used with caution in patients with cardiovascular disorders, including angina, coronary artery disease, and hypertension, and in the elderly who have a greater likelihood of occult cardiac disease. Concomitant administration of thyroid hormone and sympathomimetic agents to patients with coronary artery disease may increase the risk of coronary insufficiency.
Use of SYNTHROID in patients with concomitant diabetes mellitus, diabetes insipidus or adrenal cortical insufficiency may aggravate the intensity of their symptoms. Appropriate adjustments of the various therapeutic measures directed at these concomitant endocrine diseases may therefore be required. Treatment of myxedema coma may require simultaneous administration of glucocorticoids (see DOSAGE AND ADMINISTRATION ).
T 4 enhances the response to anticoagulant therapy. Prothrombin time should be closely monitored in patients taking both SYNTHROID and oral anticoagulants, and the dosage of anticoagulant adjusted accordingly.
Seizures have been reported rarely in association with the initiation of levothyroxine sodium therapy, and may be related to the effect of thyroid hormone on seizure threshold.
Lithium blocks the TSH-mediated release of T 4 and T 3 . Thyroid function should therefore be carefully monitored during lithium initiation, stabilization, and maintenance. If hypothyroidism occurs during lithium treatment, a higher than usual SYNTHROID dose may be required.
Information for the Patient:
Laboratory Tests: Treatment of patients with SYNTHROID requires periodic assessment of adequacy of titration by appropriate laboratory tests and clinical evaluation. Selection of appropriate tests for the diagnosis and management of thyroid disorders depends on patient variables such as presenting signs and symptoms, pregnancy, and concomitant medications. A combination of sensitive TSH assay and free T 4 estimate (free T 4 , free T 4 index) are recommended to confirm a diagnosis of thyroid disease. Normal ranges for theses parameters are age-specific in newborns and younger children.
TSH alone or initially may be useful for thyroid disease screening and for monitoring therapy for primary hypothyroidism as a linear inverse correlation exists between serum TSH and free T 4 . Measurement of total serum T 4 and T 3 , resin T 3 uptake, and free T 3 concentrations may also be useful. Antithyroid microsomal antibodies are an indicator of autoimmune thyroid disease. The presence of positive microsomal antibodies in an euthyroid patient is a major risk factor for the future development of hypothyroidism. As elevated serum TSH in the presence of normal T 4 may indicate subclinical hypothyroidism. Intracellular resistance to thyroid hormone is quite rare, and is suggested by clinical signs and symptoms of hypothyroidism in the presence of high serum T 4 levels. Adequacy of SYNTHROID therapy for hypothyroidism of pituitary or hypothalamic origin should be assessed by measuring free T 4 , which should be maintained in the upper half of the normal range. Measurement of TSH is not a reliable indicator of response to therapy for this condition. Adequacy of SYNTHROID therapy for congenital and acquired pediatric hypothyroidism should be assessed by measuring serum total T 4 or free T 4 , which should be maintained in the upper half of the normal range. In congenital hypothyroidism, normalization of serum TSH levels may lag behind normalization of serum T 4 levels by 2 or 3 months or longer. In rare patients serum TSH remains relatively elevated despite clinical euthyroidism and age-specific normal levels of T 4 or free T 4 .
Drug Interactions: The magnitude and relative clinical importance of the effects noted below are likely to be patient-specific and may vary by such factors as age, gender, race, intercurrent illnesses, dose of either agent, additional concomitant medications, and timing of drug administration. Any agent that alters thyroid hormone synthesis, secretion, distribution, effect on target tissues, metabolism, or elimination may alter the optimal therapeutic dose of SYNTHROID.
Levothyroxine sodium absorption --The following agents may bind and decrease absorption of levothyroxine sodium from the gastrointestinal tract: aluminum hydroxide, cholestyramine resin, colestipol hydrochloride, ferrous sulfate, sodium polystyrene sulfonate, soybean flour (e.g., infant formula), sucralfate.
Binding to serum proteins --The following agents may either inhibit levothyroxine sodium binding to serum proteins or alter the concentrations of serum binding proteins: androgens and related anabolic hormones, asparaginase, clofibrate, estrogens and estrogen-containing compounds, 5-fluorouracil, furosemide, glucocorticoids, meclofenamic acid, mefenamic acid, methadone, perphenazine, phenylbutazone, phenytoin, salicylates, tamoxifen.
Thyroid physiology --The following agents may alter thyroid hormone or TSH levels, generally by effects on thyroid hormone synthesis, secretion, distribution, metabolism, hormone action, or elimination, or altered TSH secretion: aminoglutethimide, p-aminosalicyclic acid, amiodarone, androgens and related anabolic hormones, complex anions (thiocyanate, perchlorate, pertechnetate), antithyroid drugs, (beta)-adrenergic blocking agents, carbamazepine, chloral hydrate, diazepam, dopamine and dopamine agonists, ethionamide, glucocorticoids, heparin, hepatic enzyme inducers, insulin, iodinated cholestographic agents, iodine-containing compounds, levodopa, lovastatin, lithium, 6-mercaptopurine, metoclopramide, mitotane, nitroprusside, phenobarbital, phenytoin, resorcinol, rifampin, somatostatin analogs, sulfonamides, sulfonylureas, thiazide diuretics.
Adrenocorticoids --Metabolic clearance of adrenocorticoids is decreased in hypothyroid patients and increased in hyperthyroid patients, and may therefore change with changing thyroid status.
Amiodarone --Amiodarone therapy alone can cause hypothyroidism or hyperthyroidism.
Anticoagulants (oral) --The hypoprothrombinemic effect of anticoagulants may be potentiated, apparently by increased catabolism of vitamin K-dependent clotting factors.
Antidiabetic agents (insulin, sulfonylureas) --Requirements for insulin or oral antidiabetic agents may be reduced in hypothyroid patients with diabetes mellitus, and may subsequently increase with the initiation of thyroid hormone replacement therapy.
(beta)-adrenergic blocking agents --Actions of some beta-blocking agents may be impaired when hypothyroid patients become euthyroid.
Cytokines (interferon, interleukin) --Cytokines have been reported to induce both hyperthyroidism and hypothyroidism.
Digitalis glycosides --Therapeutic effects of digitalis glycosides may be reduced. Serum digitalis levels may be decreased in hyperthyroidism or when a hypothyroid patient becomes euthyroid.
Ketamine --Marked hypertension and tachycardia have been reported in association with concomitant administration of levothyroxine sodium and ketamine.
Maprotiline --Risk of cardiac arrhythmias may increase.
Sodium iodide ( 123 I and 131 I), sodium pertechnetate Tc99m --Uptake of radiolabeled ions may be decreased.
Somatrem/somatropin --Excessive concurrent use of thyroid hormone may accelerate epiphyseal closure. Untreated hypothyroidism may interfere with the growth response to somatrem or somatropin.
Theophylline --Theophylline clearance may decrease in hypothyroid patients and return toward normal when a euthyroid state is achieved.
Tricyclic antidepressants --Concurrent use may increase the therapeutic and toxic effects of both drugs, possibly due to increased catecholamine sensitivity. Onset of action of tricyclics may be accelerated.
Sympathomimetic agents --Possible increased risk of coronary insufficiency in patients with coronary artery disease.
Laboratory Test Interactions: A number of drugs or moieties are known to alter serum levels of TSH, T 4 and T 3 and may thereby influence the interpretation of laboratory tests of thyroid function (see Drug Interactions ).
Carcinogenesis, Mutagenesis, and Impairment of Fertility: Although animal studies to determine the mutagenic or carcinogenic potential of thyroid hormones have not been performed, synthetic T 4 is identical to that produced by the human thyroid gland. A reported association between prolonged thyroid hormone therapy and breast cancer has not been confirmed and patients receiving levothyroxine sodium for established indications should not discontinue therapy.
Pregnancy: Pregnancy Category A. Studies in pregnant women have not shown that levothyroxine sodium increases the risk of fetal abnormalities if administered during pregnancy. If levothyroxine sodium is used during pregnancy, the possibility of fetal harm appears remote. Because studies cannot rule out the possibility of harm, levothyroxine sodium should be used during pregnancy only if clearly needed.
Thyroid hormones cross the placental barrier to some extent. T 4 levels in the cord blood of athyroid fetuses have been shown to be about one-third of maternal levels. Nevertheless, maternal-fetal transfer of T 4 may not prevent in utero hypothyroidism
Hypothyroidism during pregnancy is associated with a higher rate of complications, including spontaneous abortion and preeclampsia, and has been reported to have an adverse effect on fetal and childhood development. On the basis of current knowledge, SYNTHROID® (levothyroxine sodium, USP) should therefore not be discontinued during pregnancy, and hypothyroidism diagnosed during pregnancy should be treated. Studies have shown that during pregnancy T 4 concentrations may decrease and TSH concentrations may increase to values outside normal ranges. Postpartum values are similar to preconception values. Elevations in TSH may occur as early as 4 weeks gestation.
Pregnant women who are maintained on SYNTHROID should have their TSH measured periodically. An elevated TSH should be corrected by an increase in SYNTHROID dose. After pregnancy, the dose can be decreased to the optimal preconception dose.
Nursing Mothers: Minimal amounts of thyroid hormones are excreted in human milk. Thyroid hormones are not associated with serious adverse reactions and do not have known tumorigenic potential. While caution should be exercised when SYNTHROID is administered to a nursing woman, adequate replacement doses of levothyroxine sodium are generally needed to maintain normal lactation.
Pediatric Use: Congenital hypothyroidism: Rapid restoration of normal serum T 4 concentrations is essential for preventing the deleterious effects of neonatal thyroid hormone deficiency on intelligence, as well as on overall growth and development. SYNTHROID should be initiated immediately upon diagnosis, and is generally continued for life. The goal of therapy is to maintain the serum total T 4 or FT 4 in the upper half of the normal range and serum TSH in the normal range.
An initial starting dose of 10 to 15 mcg/kg/day (ages 0-3 months) will generally increase serum T 4 concentrations to the upper half of the normal range in less than 3 weeks. Clinical assessment of growth and development and thyroid status should be monitored frequently. In most cases, the dose of SYNTHROID per body weight will decrease gradually as the patient grows through infancy and childhood (see Table). Prolonged use of large doses in infants may be associated with later behavior problems.
Thyroid function tests (serum total T 4 or FT 4 , and TSH) should be monitored closely and used to determine the adequacy of SYNTHROID therapy. Normalization of serum T 4 levels is usually followed by a rapid decline of TSH levels. Nevertheless, normalization of TSH may lag behind normalization of T 4 levels by 2 to 3 months or longer. The relative elevation of serum TSH is more marked during the early months of therapy, but can persist to some degree throughout life. In rare patients TSH remains relatively elevated despite clinical euthyroidism and age-specific normal levels of total T 4 or FT 4 . Increasing the SYNTHROID dosage to suppress TSH into the normal range may result in overtreatment, with an elevated serum T 4 level and clinical features of hyperthyroidism, including irritability, increased appetite with diarrhea, and sleeplessness. Another risk of prolonged overtreatment in infants is premature cranial synostosis.
Assessment of permanence of hypothyroidism may be done when transient hypothyroidism is suspected. Levothyroxine therapy may be interrupted for 30 days after 3 years of age and serum measurement of T 4 and TSH levels obtained. If T 4 is low and the TSH level is elevated, permanent hypothyroidism is confirmed and therapy should be re-instituted. If T 4 and TSH remain in the normal range, a presumptive diagnosis of transient hypothyroidism can be made. In this instance, continued clinical monitoring and periodic reevaluation of thyroid function may be warranted.
Acquired hypothyroidism. The initial dose of SYNTHROID varies with age and body weight, and should be adjusted to maintain serum total T 4 or free T 4 levels in the upper half of the normal range. In general, in the absence of overriding clinical concerns, children should be started on a full replacement dose. Children with underlying heart disease should be started at lower doses, with careful upward titration. Children with severe, long-standing hypothyroidism may also be started on a lower initial dose with upward titration in an attempt to avoid premature closure of epiphyses. The recommended dose per body weight decreases with age (see Table).
Treated children may resume growth at a rate greater than normal (period of transient catch-up growth). In some cases catch-up growth may be adequate to normalize growth; however, in children with severe and prolonged hypothyroidism, adult height may be reduced. Excessive thyroxine replacement may initiate accelerated bone maturation resulting in disproportionate advancement in skeletal age and shortened adult stature.
Assessment of permanence of hypothyroidism may be done when transient hypothyroidism is suspected. Levothyroxine therapy may be interrupted for 30 days and serum measurement of T 4 and TSH levels obtained. If T 4 is low and the TSH level is elevated, permanent hypothyroidism is confirmed and therapy should be re-instituted. If T 4 and TSH remain in the normal range, a presumptive diagnosis of transient hypothyroidism can be made. In this instance, continued clinical monitoring and periodic reevaluation of thyroid function may be warranted.
Adverse reactions other than those indicative of thyrotoxicosis as a result of therapeutic overdosage, either initially or during the maintenance periods, are rare (see OVERDOSAGE ). Craniosynostosis has been associated with iatrogenic hyperthyroidism in infants receiving thyroid hormone replacement therapy. Inadequate doses of SYNTHROID may produce or fail to resolve symptoms of hypothyroidism. Hypersensitivity reactions to the product excipients, such as rash and urticaria, may occur. Partial hair loss may occur during the initial months of therapy, but is generally transient. The incidence of continued hair loss is unknown. Pseudotumor cerebri has been reported in pediatric patients receiving thyroid hormone replacement therapy.
Signs and Symptoms: Excessive doses of SYNTHROID result in a hypermetabolic state indistinguishable from thyrotoxicosis of endogenous origin. Signs and symptoms of thyrotoxicosis include weight loss, increased appetite, palpitations, nervousness, diarrhea, abdominal cramps, sweating, tachycardia, increased pulse and blood pressure, cardiac arrhythmias, tremors, insomnia, heat intolerance, fever, and menstrual irregularities. Symptoms are not always evident or may not appear until several days after ingestion.
Treatment of Overdosage: SYNTHROID should be reduced in dose or temporarily discontinued if signs and symptoms of overdosage appear.
In the treatment of acute massive SYNTHROID overdosage, symptomatic and supportive therapy should be instituted immediately. Treatment is aimed at reducing gastrointestinal absorption and counteracting central and peripheral effects, mainly those of increased sympathetic activity. The stomach should be emptied immediately by emesis or gastric lavage if not otherwise contraindicated (e.g., by coma, convulsions or loss of gag reflex). Cholestyramine and activated charcoal have also been used to decrease levothyroxine sodium absorption. Oxygen should be administered and ventilation maintained as necessary, (beta)-receptor antagonists, particularly propranolol, are useful in counteracting many of the effects of increased sympathetic activity. Propranolol may be administered intravenously at a dosage of 1 to 3 mg over a 10 minute period or orally, 80 to 160 mg/day, especially when no contraindications exist for its use. Cardiac glycosides may be administered if congestive heart failure develops. Measures to control fever, hypoglycemia, or fluid loss should be initiated as necessary. Glucocorticoids may be administered to inhibit the conversion of T 4 to T 3 .
Since T 4 is extensively protein bound, very little drug will be removed by dialysis.
The dosage and rate of administration of SYNTHROID is determined by the indication, and must in every case be individualized according to patient response and laboratory findings.
Hypothyroidism: The goal of therapy for primary hypothyroidism is to achieve and maintain a clinical and biochemical euthyroid state with consequent resolution of hypothyroid signs and symptoms. The starting dose of SYNTHROID, the frequency of dose titration, and the optimal full replacement dose must be individualized for every patient, and will be influenced by such factors as age, weight, cardiovascular status, presence of other illness, and the severity and duration of hypothyroid symptoms.
The usual full replacement dose of SYNTHROID for younger, healthy adults is approximately 1.6 mcg/kg/day administered once daily. In the elderly, the full replacement dose may be altered by decreases in T 4 metabolism and levothyroxine sodium absorption. Older patients may require less than 1 mcg/kg/day. Children generally require higher doses (see Pediatric Dosage ). Women who are maintained on SYNTHROID during pregnancy may require increased doses (see Pregnancy ).
Therapy is usually initiated in younger, healthy adults at the anticipated full replacement dose. Clinical and laboratory evaluations should be performed at 6 to 8 week intervals (2 to 3 weeks in severely hypothyroid patients), and the dosage adjusted by 12.5 to 25 mcg increments until the serum TSH concentration is normalized and signs and symptoms resolve. In older patients or in younger patients with a history of cardiovascular disease, the starting dose should be 12.5 to 50 mcg once daily with adjustments of 12.5 to 25 mcg every 3 to 6 weeks until TSH is normalized. If cardiac symptoms develop or worsen, the cardiac disease should be evaluated and the dose of SYNTHROID reduced. Rarely, worsening angina or other signs of cardiac ischemia may prevent achieving a TSH in the normal range.
Treatment of subclinical hypothyroidism, when indicated, may require lower than usual replacement doses, e.g. 1.0 mcg/kg/day. Patients for whom treatment is not initiated should be monitored yearly for changes in clinical status, TSH, and thyroid antibodies.
In patients with hypothyroidism resulting from pituitary or hypothalamic disease, the possibility of secondary adrenal insufficiency should be considered, and if present, treated with glucocorticoids prior to initiation of SYNTHROID. The adequacy of SYNTHROID therapy should be assessed in these patients by measuring FT 4 I, which should be maintained in the upper half of the normal range, in addition to clinical assessment. Measurement of TSH is not a reliable indicator of response to therapy for this condition.
Few patients require doses greater than 200 mcg/day. An inadequate response to daily doses of 300 to 400 mcg/day is rare, and may suggest malabsorption, poor patient compliance, and/or drug interactions.
Once optimal replacement is achieved, clinical and laboratory evaluations should be conducted at least annually or whenever warranted by a change in patient status. Levothyroxine sodium products from different manufacturers should not be used interchangeably unless retesting of the patient and retitration of the dosage, as necessary, accompanies the product switch.
SYNTHROID Injection by the intravenous of intramuscular route can be substituted for the oral dosage form when the oral administration is precluded. The initial parenteral dosage should be approximately one-half the previously established oral dosage of SYNTHROID Tablets. Close observation of the patient is recommended, with adjustment of the dosage as needed. Administration of SYNTHROID Injection by the subcutaneous route is not recommended as studies have shown that the influx of T 4 from the subcutaneous site is very slow, and depends on many factors such as volume of injectate, the anatomic site of injection, ambient temperature, and presence of venospasm.
Myxedema Coma: Myxedema coma represents the extreme expression of severe hypothyroidism and is considered a medical emergency. It is characterized by hypothermia, hypotension, hypoventilation, hyponatremia, and bradycardia. In addition to restoration of normal thyroid hormone levels, therapy should be directed at the correction of electrolyte disturbances and possible infection. Because the mortality rate of patients with untreated myxedema coma is high, treatment must be started immediately, and should include appropriate supportive therapy and corticosteroids to prevent adrenal insufficiency. Possible precipitating factors should also be identified and treated. SYNTHROID may be given via nasogastric tube, but the preferred route of administration is intravenous. A bolus dose of SYNTHROID is given immediately to replete the peripheral pool of T 4 , usually 300 to 500 mcg. Although such a dose is usually well-tolerated even in the elderly, the rapid intravenous administration of large doses of levothyroxine sodium to patients with cardiovascular disease is clearly not without risks. Under such circumstances, intravenous therapy should not be undertaken without weighing the alternate risks of myxedema coma and the cardiovascular disease. Clinical judgement in this situation may dictate smaller intravenous doses of SYNTHROID. The initial dose is followed by daily intravenous doses of 75 to 100 mcg until the patient is stable and oral administration is feasible. Normal T 4 levels are usually achieved in 24 hours, followed by progressive increases in T 3 . Improvement in cardiac output, blood pressure, temperature, and mental status generally occur within 24 hours, with improvement in many manifestations of hypothyroidism in 4 to 7 days.
TSH Suppression in Thyroid Cancer and Thyroid Nodules: The rationale for TSH suppression therapy is that a reduction in TSH secretion may decrease the growth and function of abnormal thyroid tissue. Exogenous thyroid hormone may inhibit recurrence of tumor growth and may produce regression of metastases from well-differentiated (follicular and papillary) carcinoma of the thyroid. It is used as ancillary therapy of these conditions following surgery or radioactive iodine therapy. Medullary and anaplastic carcinoma of the thyroid is unresponsive to TSH suppression therapy. TSH suppression is also used in treating nontoxic solitary nodules and multinodular goiters.
No controlled studies have compared the various degrees of TSH suppression in the treatment of either benign or malignant thyroid nodular disease. Further, the effectiveness of TSH suppression for benign nodular disease is controversial. The dose of SYNTHROID used for TSH suppression should therefore be individualized by the nature of the disease, the patient being treated, and the desired clinical response, weighing the potential benefits of therapy against the risks of iatrogenic thyrotoxicosis. In general, SYNTHROID should be given in the smallest dose that will achieve the desired clinical response.
For well-differentiated thyroid cancer, TSH is generally suppressed to less than 0.1 mU/L. Doses of SYNTHROID greater than 2 mcg/kg/day are usually required. The efficacy of TSH suppression in reducing the size of benign thyroid nodules and in preventing nodule regrowth after surgery are controversial. Nevertheless, when treatment with levothyroxine sodium is considered warranted, TSH is generally suppressed to a higher target range (e.g., 0.1 to 0.3 mU/L) than that employed for the treatment of thyroid cancer. SYNTHROID therapy may also be considered for patients with nontoxic multinodular goiter who have a TSH in the normal range, to moderately suppress TSH (e.g., 0.1 to 0.3 mU/L).
SYNTHROID should be administered with caution to patients in whom there is a suspicion of thyroid gland autonomy, in view of the fact that the effects of exogenous hormone administration will be additive to endogenous thyroid hormone production.
Pediatric Dosage: Congenital or acquired hypothyroidism: The dosage of SYNTHROID for pediatric hypothyroidism varies with age and body weight. SYNTHROID should be given at a dose that maintains the serum total T 4 or free T 4 concentrations in the upper half of the normal range and serum TSH in the normal range (see Pediatric Use ).
SYNTHROID therapy is usually initiated at the full replacement dose (see Table). Infants and neonates with very low or undetectable serum T 4 levels (<5 mcg/dL) should start at the higher end of the dosage range (e.g., 50 mcg daily). A lower starting dosage (e.g., 25 mcg daily) should be considered for neonates at risk of cardiac failure, increasing every few days until a full maintenance dose is reached. In children with severe, long-standing hypothyroidism, SYNTHROID should be initiated gradually, with an initial dose of 25 mcg for two weeks, and then increasing the dose by 25 mcg every 2 to 4 weeks until the desired dose based on serum T 4 and TSH levels is achieved. (see Pediatric Use ).
Serum T 4 and TSH measurements should be evaluated at the following intervals, with subsequent dosage adjustments to normalize serum total T 4 or FT 4 , and TSH:
2 and 4 weeks after the initiation of SYNTHROID treatment;
every 1 to 2 months during the first year of life;
every 2 to 3 months between 1 and 3 years of age;
every 3 to 12 months thereafter until growth is completed.
Evaluation at more frequent intervals is advisable when compliance is questioned or abnormal values are obtained. Patient evaluation is also advisable approximately 6 to 8 weeks after any change in SYNTHROID dose.
SYNTHROID tablets may be given to infants and children who cannot swallow intact tablets by crushing the tablet and suspending the freshly crushed tablet in a small amount of water (5 to 10 mL), breast milk or non-soybean formula. The suspension can be given by spoon or dropper. DO NOT STORE THE SUSPENSION FOR ANY PERIOD OF TIME. The crushed tablet may also be sprinkled over a small amount of food, such as apple sauce. Foods or formula containing large amounts of soybean, fiber, or iron should not be used for administering SYNTHROID.
|
||||||||||||||||||||
SYNTHROID® (levothyroxine sodium, USP) Tablets: round, color coded, scored tablet debossed with "FLINT" and potency.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Store at controlled room temperature 15°-30°C (59°-86°F). SYNTHROID Tablets should be protected from light and moisture.
SYNTHROID® (levothyroxine sodium, USP) Injection is a lyophilized powder. It is supplied in color coded vials as follows:
|
||||||||
Store at controlled room temperature 15°- 30C (59 - 86°F).
DIRECTIONS FOR RECONSTITUTION: Reconstitute the lyophilized levothyroxine sodium by aseptically adding 5 mL of 0.9% Sodium Chloride Injection, USP (final volume approximately 5mL). Shake vial to insure complete mixing. Do not add to other intravenous fluids. Use immediately after reconstitution. Discard any unused portion.
CAUTION: Federal (USA) law prohibits dispensing without a prescription.
Tablets Manufactured by
BASF Pharmaceuticals
A Unit of BASF
Jayuya, Puerto Rico 00664
Injection Manufactured by
Ben Venue Laboratories, Inc.
Bedford, Ohio 44146 USA
For
Knoll Pharmaceutical Company
3000 Continential Drive-North
BASF Pharma
©1998 Knoll Pharmaceutical Company
SYNTHROID is a registered trademark of Knoll
Pharmaceutical Company
Revised: April 1998 7920-10
 |
 |